
The LateralNeck
Some photos from Loren G. Yamamoto, MD of the University of Hawaii
© Copyright William Herring, MD, FACR
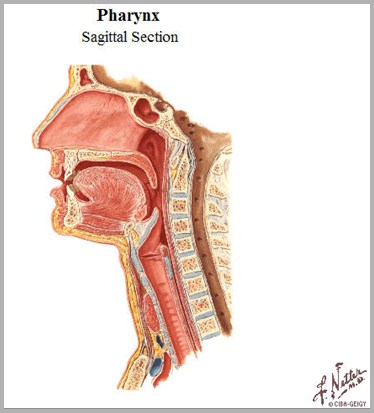
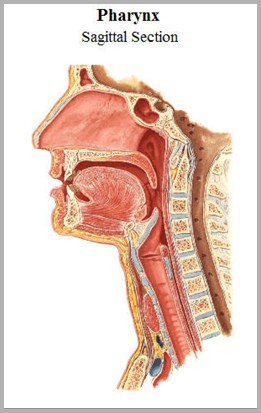
Nasopharynx
Oropharynx
Hypopharynx
Glottis
Trachea
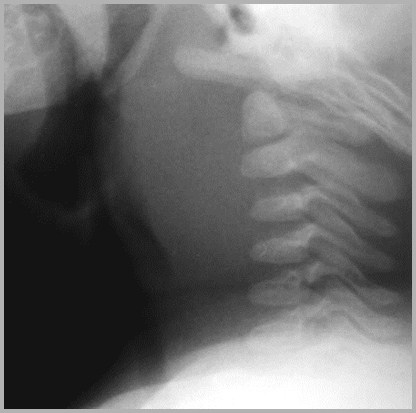
Normal

Normal Adult
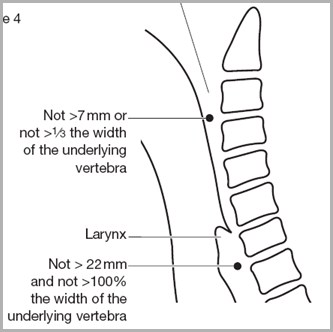
Soft tissues
At C3: <3 mm (less than 1/3 AP diameter)
At C6: < the AP width of C6 vertebral body
Predentate space
< 3mm
Normal Adult
3
6

33
33
66
66
Herring’s 3 rules of 3
The predentate space should be < 3mm
The prevertebral soft tissue at C3 isusually 3 mm
Anterior wedging of 3mm or moresuggests a fx of that vertebral body
Normal Child
Predentate space < 5 mm
Straightening of the spine iscommon
C2 may appear subluxed on C3
Laryngeal cartilage calcificationis pathologic in children(relapsing polychondritis)
Adenoids are invisible until 6mos and regress after 6 years
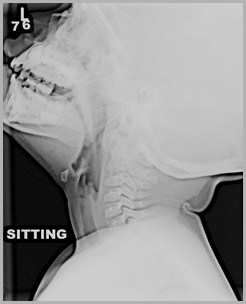
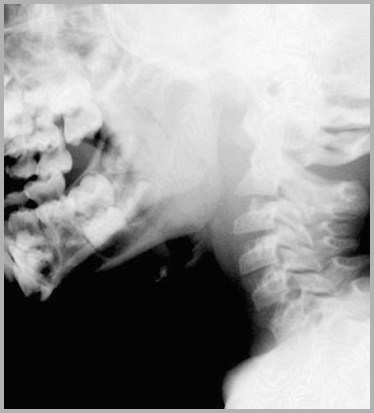
Head extended, full inspiration

Images taken withhead flexed or inexpiration will causespuriousenlargement of theretropharyngeal softtissues
Flexion versus Extension

Soft tissues look enlarged
Soft tissues normal
Head flexedHead flexed
Head extendedHead extended
35 Words About Adenoids
Invisible until 3-6 months
Newborns do not have visibleadenoids
Pathological when they encroachon nasopharyngeal airway
They can grow until about age 6
They involute in adulthood
Adults do not have visibleadenoids
Measurements are not reliable

9 year-old
Revenge of the Noids
If no adenoidal tissue after 6 months
Suspect immune deficiency
If enlarged adenoids after childhood
Suspect lymphatic malignancy
Lymphoma
Leukemia

Enlarged Tonsils and Adenoids
R3
Adenoids
LingualTonsils
Enlarged Adenoids/Tonsils
Associated with
Nasal congestion
Chronic or recurrent otitis media
Painful swallowing
Sleep apnea
Treatment
Wait until they involute
Surgically remove them
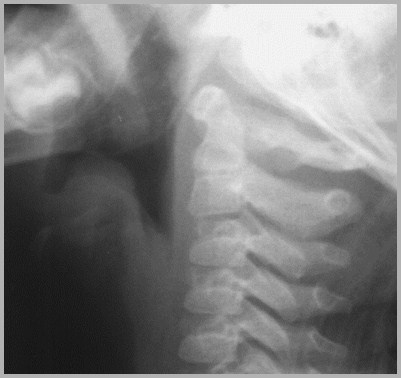
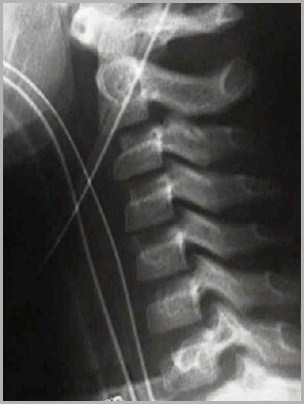
Pseudo versus True Subluxation
Posterior cervical line
Connects spinolaminarline of C1 and C3
Should pass within 2mm of spinolaminar lineof C2


Pseudosubluxation
Mostpronouncedwith headflexed
If subluxationpersists onextensionview=truesubluxation
Pseudo-subluxation willonly occur withthe neck inflexion
C2
C3

Hangman’s Fracture
What’s this?
Retropharyngeal Space
Contains lymphatics that drain
Nasopharynx
Adenoids
Posterior nasal sinuses
These chains atrophy after age 4
Retropharyngeal Abscess
Almost all occur before age 6
50% between 6-12 months
Most common pathogens are
Staph aureus
Group A Beta hemolytic Strep
Hemophilus
Retropharyngeal Abscess
Clinically
Prodromal nasopharyngitis
Severe throat pain with drooling
Dysphagia
Hyperextension of the head
“Hot potato” muffled voice
In adults, usually 2° trauma to oropharynx
Iatrogenic
Perforated FB

Retropharyngeal Abscess

Some photos from Loren G. Yamamoto, MD of the University of Hawaii

Retropharyngeal Abscess
Retropharyngeal AbscessRole of CT
Plain film is usually adequate to make dx
CT useful in
Distinguishing abscess from phlegmon
Determining extent of abscess
Localizing lesion
Determine which deep neck spaces are involved
Retropharyngeal Perforation
Causes
Trauma to esophagus or trachea
Penetrating injuries from weapons
Perforation from within
•Chicken bone
Mediastinal emphysema tracking into neck
Retropharyngeal abscess 2° gas-formingorganism
Retropharyngeal Perforation
Imaging findings
Streaks of air in soft tissues of neck
Anterior displacement of pharynx
Associated pneumothorax possible
Cervical or mediastinal air seen in 60% ofcases of ruptured esophagus
Retropharyngeal Air


Retropharyngeal Abscess from Chicken Bone


Turkey Bone-Before and After
Upper Airway Infections
The Big Two
Croup
Epiglottitis
Croup
Laryngotrachealbronchitis
Usually viral
May be difficult to distinguish from earlyretropharyngeal abscess
Occurs at age 6 months to 2 years
Younger than epiglottitis
Croup
The three major findings of croup
Distension of the hypopharynx
Distension of the laryngeal ventricle
Haziness or narrowing of subglottic space

Croup
Dilatation of thehypopharynx
Distension ofthe laryngealventricle
Narrowing ofsub-glotticarea
Croup
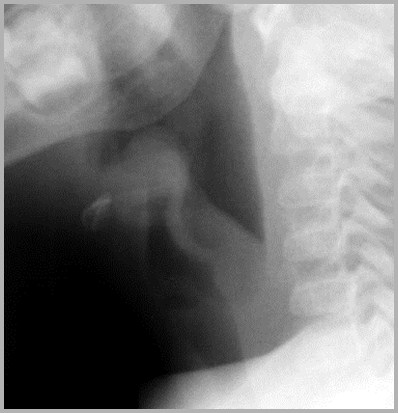
Epiglottitis
Most commonly H. flu type B
Peak incidence now closer to 6-7 years
Croup occurs from 6 months to 2 years
Lateral radiograph -- erect position only
Supine position may close off airway
Epiglottitis
Imaging findings
Epiglottis is enlarged
Appears thumb-like
Aryepiglottic folds are thickened
Pre-epiglottic space (vallecula) is smallerthan normal
In many cases, it’s obliterated

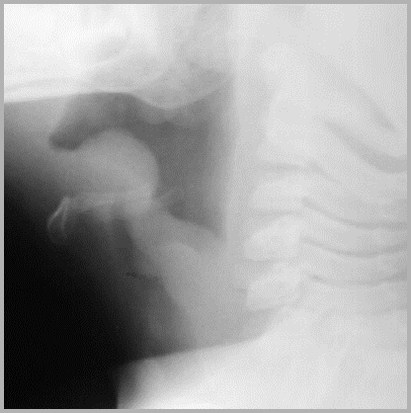
Acute Epiglottitis
Enlargementof epiglottis“thumb sign”
Thickeningof thearyepiglotticfolds
Narrowingof the pre-epiglotticspace(vallecula)
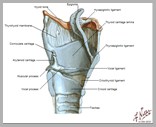
Aryepiglottic Fold
Extend betweenarytenoid cartilage andlateral margin ofepiglottis on each side
Constitute lateralborders of laryngealinlet

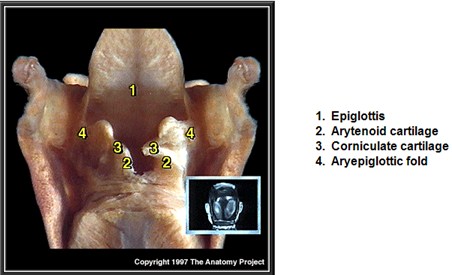

Gross Anatomy-Aryepiglottic Folds

A
P
Gross Anatomy-Aryepiglottic Folds
Acute Epiglottitis
Enlargedaryepiglotticfolds
Thumb-likeepiglottis
Cervical Masses/Hematomas
Cystic hygroma
Hemangioma
Neuroblastoma
Neurofibroma
Myxedema
Foreign body
Traumatic instrumentation
Cervical spine injury
Lymphoma, leukemia
Infectious mononucleosis
Tuberculosis
Leukemia-Posterior Pharyngeal Mass
Waldeyer’s Ring
Adenoids
Palatine tonsils
Lingual tonsils
Foreign BodiesImpacted
Food or true foreign bodies
Chicken bones (opaque), fish bones (non-opaque)
Coins, trucks
Impact just below cricopharyngeous (70%)
20% at aortic arch
10% at EG junction
Dysphagia and odynophagia
Nearly all move though GI tract once passed esophagus
Always check for lead lines in children
Pica

Esophagus
Trachea
Most coins willnot fit in thetrachea

Chickenbones areusuallyopaque
Fish bonesare not
Even if FBpasses,manycomplain ofpain in neck
Fractures and Dislocations
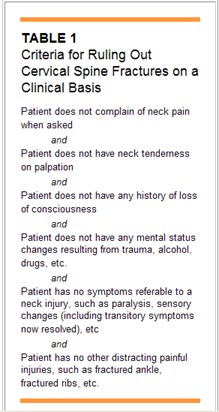
American Academyof Family PhysiciansJanuary, 1999
Soft Tissues and Fractures
“Prevertebral soft tissue measurementat C3 is an insensitive marker ofcervical spine fracture or dislocationand does not correlate with the locationor mechanism of injury”
If soft tissue swelling is present, likelihood of fx or ligamentous injury
Am J Emerg Med. 1998 Jul;16(4):346-9

Compression fractures C4 and C5 – No significant swelling

Fracture of Odontoid – Massive swelling
Atlanto-axial DislocationMassive Swelling

Things that look likediseases but aren’t
Normal variant

Fx?
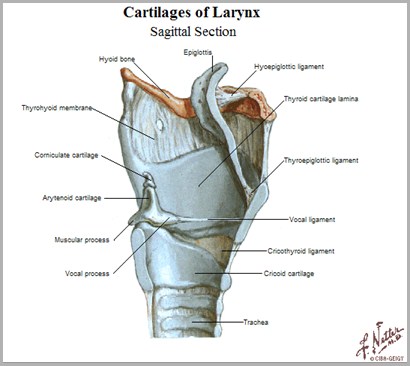
Larynx

Tumor?

Tongue
Tonsils?

Flexed, not extended, head
Retropharyngealabscess?

Cricoid cartilage
Foreign body?

Earlobe
Tumor?

Unknowns
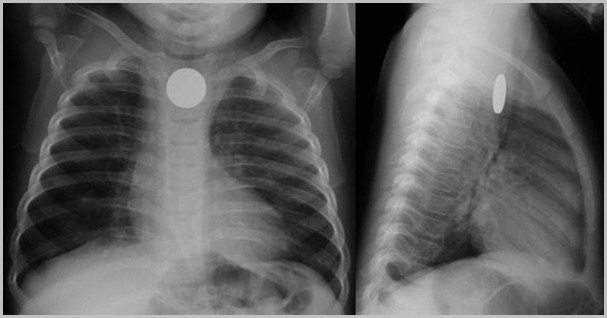
Coin Impacted in esophagus

Acute Epiglottitis
Retropharyngeal Abscess

Pseudosubluxation

Retropharyngeal Abscess
Enlarged Adenoids

2 year-old

Retropharyngeal Air

Acute Epiglottitis

Croup
Enlarged tonsils and adenoids

3 year-old

Fractured larynx

Acute Epiglottitis

FB with abscess
R3

Retropharyngeal Abscess
Acute Epiglottitis

Retropharyngeal Abscess from Chicken Bone

Enlarged tonsils and adenoids
R3
5 year-old
Pseudosubluxation
Wheeless’ Orthopedics

Retropharyngeal Abscess



Zenker’s Diverticulum
Enlarged tonsils

11 year-old11 year-old
Acute Epiglottitis
The End